
Imagine picking up a prescription at the pharmacy and seeing a familiar blue bottle, but with a different label and a price tag that is a fraction of what you expected. You might wonder: "Is this actually going to work?" It is a fair question. For decades, patients have trusted that generic drugs are medications that contain the same active ingredients as brand-name drugs but are sold under their chemical names or the manufacturer's name. But how can you be sure they perform identically inside your body? The answer lies not in guesswork, but in a rigorous scientific framework enforced by the U.S. Food and Drug Administration (FDA). This system ensures that every generic pill you take meets the exact same high standards for safety, strength, and quality as the original brand-name medication.
The Legal Foundation: The Hatch-Waxman Act
To understand how generics are approved today, we have to look back to 1984. Before then, the pharmaceutical landscape was dominated by expensive brand-name monopolies. Congress passed the Drug Price Competition and Patent Term Restoration Act, commonly known as the Hatch-Waxman Act. This legislation created a balanced pathway. It allowed generic manufacturers to enter the market without repeating costly and time-consuming clinical trials that had already proven the drug’s safety and efficacy. In exchange, it extended patent protections for innovator brands to compensate for time lost during regulatory review. This act established the legal mechanism for the Abbreviated New Drug Application (ANDA), which remains the cornerstone of generic drug approval today.
The ANDA Process: Proving Equivalence Without Redundancy
When a company wants to sell a generic version of a brand-name drug, they submit an ANDA to the FDA’s Office of Generic Drugs (OGD). Unlike a New Drug Application (NDA) for a brand-new medication, which requires years of animal studies and human clinical trials, the ANDA is "abbreviated." The manufacturer relies on the FDA’s previous finding that the reference listed drug (RLD)-the original brand-is safe and effective. Their job is to prove that their product is therapeutically equivalent to that RLD. This means demonstrating that the generic drug has the identical active ingredient, strength, dosage form, and route of administration. The process typically takes 3 to 5 years from initial development to approval, costing between $1.5 million and $3 million for standard products, though complex generics like inhalers can cost up to $25 million due to intricate testing requirements.
Bioequivalence: The Scientific Gold Standard
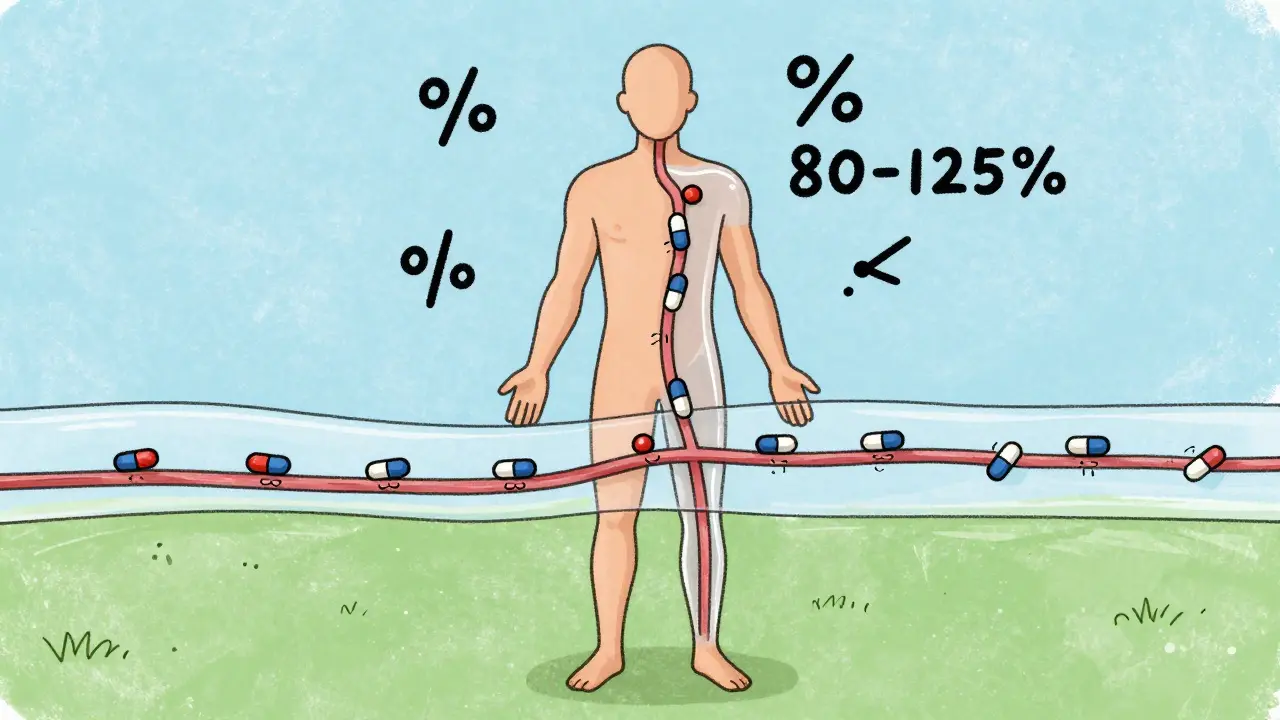
The heart of the FDA’s assurance is a concept called bioequivalence. This is not just a vague promise; it is a precise mathematical requirement. Manufacturers must conduct clinical studies, usually involving 24 to 36 healthy volunteers, to show that the rate and extent of absorption of the generic drug into the bloodstream fall within a strict range compared to the brand. Specifically, the 90% confidence interval of the geometric mean ratios for two key metrics-AUC (area under the curve, representing total exposure) and Cmax (maximum concentration)-must fall between 80% and 125%. If a generic drug absorbs too quickly or too slowly, it fails this test. For narrow therapeutic index drugs, such as levothyroxine or warfarin, where small changes in blood levels can be dangerous, the FDA applies even tighter criteria, requiring the ratio to fall between 90% and 111%.
| Requirement | Brand-Name Drug (NDA) | Generic Drug (ANDA) |
|---|---|---|
| Active Ingredient | Must be novel and proven safe/effective | Must be identical to the Reference Listed Drug |
| Clinical Trials | Extensive Phase I-III human trials required | Bioequivalence study only (no full clinical trials) |
| Strength & Dosage | Determined during development | Must match RLD exactly (±5% tolerance) |
| Review Timeline | Typically 10+ months, often longer | Targeted at 10 months (GDUFA II goal) |
| Cost to Develop | $1 billion+ average | $1.5 million - $3 million (standard) |
Manufacturing Quality and cGMP Compliance
Proving equivalence in a lab is only half the battle. The FDA also ensures that every single pill produced meets these standards through Current Good Manufacturing Practices (cGMP), codified in 21 CFR Parts 210 and 211. These regulations require manufacturers to validate their production processes to ensure batch-to-batch consistency. Facilities undergo annual inspections, and any deviation can result in a Complete Response Letter (CRL), halting the approval process. According to FDA data, manufacturing process issues account for 22% of all CRLs issued. Furthermore, while inactive ingredients (like fillers or dyes) may differ between generic and brand versions, they must be present in safe quantities as defined by the FDA’s Inactive Ingredient Database. The final product must meet USP <905> uniformity standards, ensuring that each tablet contains between 85% and 115% of the labeled amount of active ingredient.
Real-World Performance and Patient Safety
Does this rigorous process translate to real-world results? Data suggests yes. A 2023 analysis by the IQVIA Institute examined 15 million patient records and found no statistically significant difference in clinical outcomes between brand-name and generic versions of 20 common medications, including atorvastatin and metformin. In fact, adherence rates were 3.2% higher for generics, largely because lower out-of-pocket costs make it easier for patients to stay on their medication. The FDA’s Adverse Event Reporting System (FAERS) shows nearly identical safety profiles, with 1.7 adverse event reports per million prescriptions for generics versus 1.6 for brands. However, some experts note exceptions. Dr. Randall Stafford of Stanford University highlighted concerns about narrow therapeutic index drugs, where 11% of physicians reported clinical concerns about substitution. To address this, the FDA maintains a specific list of Narrow Therapeutic Index Drug Products, applying stricter oversight to ensure patient safety.
Economic Impact and Market Dynamics
The success of the FDA’s generic approval process has profound economic implications. Generic drugs now account for approximately 90% of all prescriptions dispensed in the United States, yet they represent only 23% of total pharmaceutical spending. This disparity saves the American healthcare system an estimated $313 billion annually, according to the Association for Accessible Medicines. Major players like Teva Pharmaceutical Industries, Viatris, and Sandoz dominate the market, but the FDA’s Generic Drug Competition Action Plan has helped smaller manufacturers gain ground, addressing shortages and fostering competition. With major blockbusters like Humira losing patent protection, the global generic pharmaceuticals market is projected to grow at 6.8% annually through 2028, driven by the FDA’s streamlined pathways and initiatives like GDUFA III, which aims to reduce review times to 8 months for standard applications.
Addressing Common Misconceptions
Despite the evidence, skepticism persists. A 2021 survey found that 37% of independent pharmacists reported patients expressing concerns about generic efficacy. Often, these concerns stem from visible differences in appearance-color, shape, or size-which are determined by inactive ingredients. Patients may also experience the "nocebo effect," where expecting a worse outcome leads to perceived side effects. The FDA addresses this by allowing different inactive ingredients as long as they do not affect the drug’s performance. For complex products like topical creams or inhalers, where delivery mechanisms are more intricate, the FDA has issued specific guidances to ensure equivalence. Understanding that the active ingredient-the part that treats the disease-is identical helps bridge the gap between perception and reality.
Are generic drugs really as effective as brand-name drugs?
Yes. The FDA requires generic drugs to demonstrate bioequivalence, meaning they deliver the same amount of active ingredient into your bloodstream in the same amount of time as the brand-name drug. Clinical studies and real-world data consistently show no significant difference in effectiveness or safety for the vast majority of medications.
Why do generic drugs look different from brand-name drugs?
Generic drugs can have different colors, shapes, or sizes because they may use different inactive ingredients (excipients) like fillers, binders, or dyes. These inactive ingredients do not affect the therapeutic action of the drug. The active ingredient, which provides the medical benefit, must be identical to the brand-name version.
What is bioequivalence?
Bioequivalence is a measure used by the FDA to ensure that a generic drug performs similarly to its brand-name counterpart in the body. It requires that the rate and extent of absorption of the generic drug fall within 80-125% of the brand-name drug’s profile. This statistical range ensures that any differences are not clinically meaningful.
Can I switch between different generic manufacturers?
In most cases, yes. All FDA-approved generics for the same drug are considered therapeutically equivalent. Pharmacists often substitute one generic manufacturer for another based on availability and cost. However, for narrow therapeutic index drugs (like certain seizure or thyroid medications), doctors may prefer to keep patients on a specific manufacturer to maintain consistent blood levels.
How much does it cost to develop a generic drug?
Developing a typical generic drug costs between $1.5 million and $3 million and takes 3 to 5 years. This is significantly less than the $1 billion+ average cost to develop a new brand-name drug, which involves extensive preclinical and clinical trials. Complex generics, such as inhalers or injectables, can cost up to $25 million due to more challenging bioequivalence studies.