DOAC Dosing Calculator for Renal Impairment
When someone has atrial fibrillation and also has kidney problems, choosing the right blood thinner isn’t just about picking a pill-it’s about getting the dose just right. Too much can cause dangerous bleeding. Too little can lead to a stroke. Direct Oral Anticoagulants (DOACs) like apixaban, a direct factor Xa inhibitor used to prevent stroke in patients with atrial fibrillation, rivaroxaban, an oral anticoagulant that blocks factor Xa to reduce blood clot formation, dabigatran, a direct thrombin inhibitor approved for stroke prevention in non-valvular atrial fibrillation, and edoxaban, a factor Xa inhibitor with once-daily dosing for atrial fibrillation and deep vein thrombosis are now the go-to options for most patients. But if their kidneys aren’t working well, these drugs can build up in the body and turn from lifesavers into serious risks.
Why Kidney Function Changes Everything
Unlike warfarin, which the liver breaks down, DOACs leave the body mostly through the kidneys. If your kidneys are weak, the drug stays in your system longer. That’s not a problem if you’re healthy. But if your creatinine clearance (CrCl) drops below 30 mL/min, you’re in danger zone. Studies show that over 40% of people with atrial fibrillation also have some level of chronic kidney disease. And for those on dialysis? The numbers get even more complicated.
The key is not to rely on eGFR numbers you see on lab reports. Doctors must use the Cockcroft-Gault formula, a method to estimate creatinine clearance based on age, weight, sex, and serum creatinine. It’s old-developed in 1976-but it’s still the gold standard for DOAC dosing. Why? Because the FDA and major guidelines specifically require it. Using eGFR instead can lead to over- or under-dosing. And that’s not theoretical. A 2022 study in JAMA Internal Medicine found that nearly 37% of DOAC prescriptions in patients with kidney disease were dosed incorrectly.
How Each DOAC Is Adjusted
Not all DOACs handle kidney problems the same way. Here’s what actually works in practice:
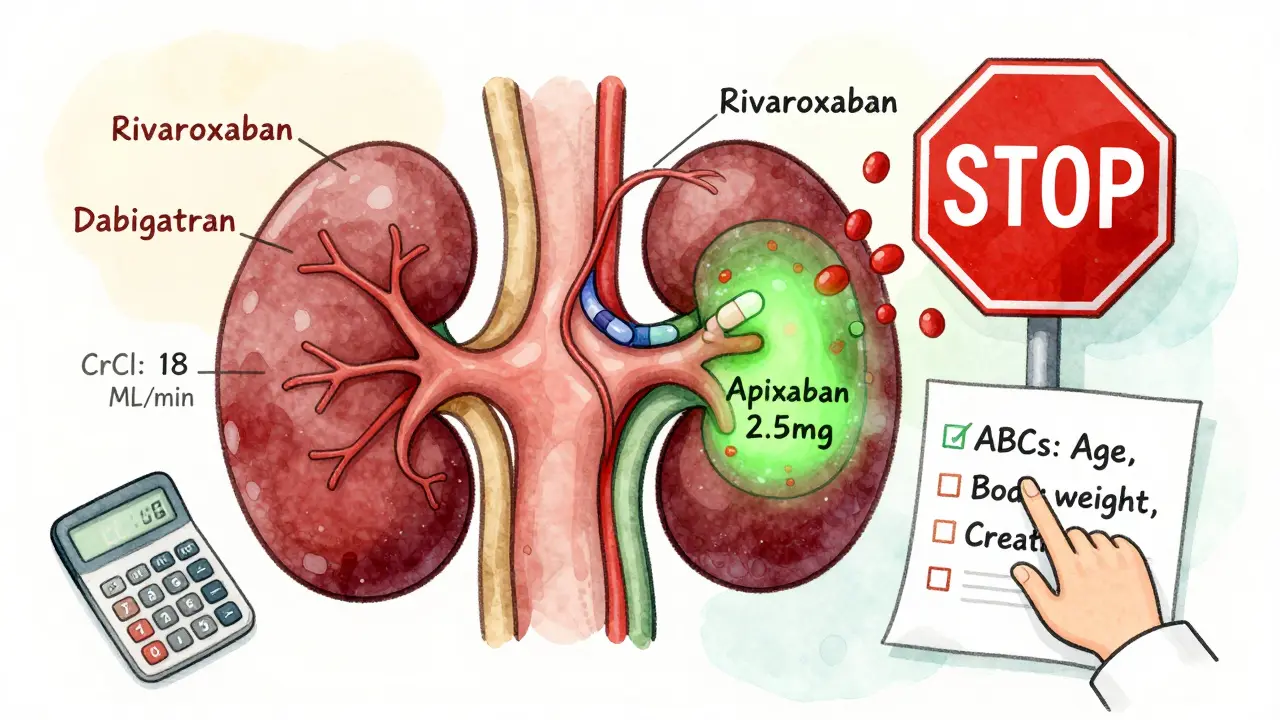
- Apixaban: Standard dose is 5 mg twice daily. But if you’re 80 or older, weigh 60 kg or less, or have a serum creatinine of 1.5 mg/dL or higher, you drop to 2.5 mg twice daily. If your CrCl is below 15 mL/min, it’s not approved-but many nephrologists still use 2.5 mg twice daily in dialysis patients, and early data suggests it’s safer than warfarin.
- Rivaroxaban: Should never be used if CrCl is below 15 mL/min. Even at 15-29 mL/min, the dose drops to 15 mg once daily. But in real-world use, many doctors avoid it altogether in advanced kidney disease because the risk of bleeding climbs sharply.
- Dabigatran: Dose drops from 150 mg to 75 mg twice daily when CrCl is between 15 and 30 mL/min. Below 15 mL/min? Avoid it. It’s the most dependent on kidney clearance of all the DOACs.
- Edoxaban: Standard dose is 60 mg once daily. Drop to 30 mg once daily if CrCl is between 15 and 50 mL/min. Below 15 mL/min? Not approved. It’s less studied in dialysis patients than apixaban.
Apixaban stands out. It’s the only DOAC with FDA approval for use in patients on hemodialysis-even though it’s not officially labeled for that use. A 2020 review in the Journal of the American Heart Association found apixaban had lower bleeding rates than warfarin in patients with end-stage kidney disease. In one clinic, doctors tracked 127 dialysis patients on apixaban 2.5 mg twice daily for 18 months. Their major bleeding rate was 1.8%. In their warfarin group? 3.7%.
The ABCs of Apixaban Dosing
For apixaban, doctors use a simple memory trick: ABCs.
- Age ≥80 years
- Body weight ≤60 kg
- Creatinine ≥1.3 mg/dL (or 133 μmol/L)
If two or more of these apply, reduce the dose. This isn’t just a rule of thumb-it’s based on clinical trial data. One 78-year-old woman weighing 55 kg with a creatinine of 1.6 mg/dL was prescribed 5 mg twice daily. She ended up in the ER with a life-threatening GI bleed. Her CrCl was 18 mL/min. She should’ve been on 2.5 mg. This isn’t rare. Pharmacists report that 28% of Cockcroft-Gault calculations in patients over 80 need manual adjustment because of low muscle mass or frailty. The formula doesn’t always account for that.
What About Dialysis Patients?
This is where things get murky. There’s no clear consensus. The 2023 KDIGO guidelines say there’s still “lack of quality evidence” for any DOAC in patients on hemodialysis. But real-world experience is shifting. Apixaban is being used off-label in dialysis units across the U.S. and Europe. Rivaroxaban and dabigatran? Avoided. Edoxaban? Too little data.
Here’s what we know: Warfarin isn’t the answer either. Studies show it causes more intracranial bleeds and vascular calcification in dialysis patients. A 2020 review called warfarin’s use in ESRD “little proven benefit and a large risk of harm.” So even though the evidence isn’t perfect, apixaban is becoming the default choice for dialysis patients with atrial fibrillation. The ongoing RENAL-AF trial, expected to finish in 2025, may finally give us solid answers.
Common Mistakes and How to Avoid Them
Here’s what goes wrong-and how to fix it:
- Mistake: Using eGFR instead of CrCl. Fix: Always calculate CrCl using Cockcroft-Gault. Write it down on the prescription.
- Mistake: Assuming all DOACs are the same. Fix: Know the specific rules for each drug. Apixaban can be used in dialysis. Rivaroxaban cannot.
- Mistake: Not checking kidney function after starting. Fix: Recheck CrCl every 3-6 months. If it drops, reassess the dose.
- Mistake: Prescribing standard dose to elderly, low-weight patients. Fix: Use the ABCs for apixaban. If in doubt, start low.
Virtual anticoagulation clinics have helped cut errors by 22%. These are remote teams-often pharmacists and nurses-who monitor labs, flag dose issues, and call doctors when something looks off. In a world where 37% of prescriptions are wrong, that kind of system isn’t optional anymore.
What’s Next?
By 2026, we’ll likely have clearer guidelines for every stage of kidney disease, including dialysis. The AXIOS trial, though small, will release data on apixaban’s pharmacodynamics in dialysis patients in late 2024. The RENAL-AF trial, comparing apixaban to warfarin in severe kidney disease, will report in 2025. Until then, the safest approach is simple:
- If CrCl >30 mL/min: Any DOAC is fine. No adjustment needed.
- If CrCl 15-30 mL/min: Use apixaban 2.5 mg twice daily or edoxaban 30 mg daily. Avoid dabigatran and rivaroxaban.
- If CrCl <15 mL/min or on dialysis: Apixaban 2.5 mg twice daily is the best option we have. Avoid the others.
DOACs are better than warfarin for most people. But in kidney disease, they’re not one-size-fits-all. Getting it right means knowing the numbers, knowing the drug, and never assuming.
Can I use any DOAC if I’m on dialysis?
No. Only apixaban is commonly used and supported by emerging data in dialysis patients. Rivaroxaban, dabigatran, and edoxaban are not recommended. Apixaban is typically dosed at 2.5 mg twice daily, even though it’s not officially labeled for dialysis. Always confirm with a nephrologist or anticoagulation specialist.
Why is Cockcroft-Gault used instead of eGFR for DOAC dosing?
Because the FDA and major guidelines specifically require it. The Cockcroft-Gault formula estimates creatinine clearance based on weight, age, sex, and serum creatinine, which better reflects how much drug the kidneys can clear. eGFR estimates filtration rate but doesn’t account for body size the same way. Using eGFR can lead to overestimating kidney function and overdosing, especially in elderly or underweight patients.
Is apixaban really safer than warfarin in kidney disease?
Yes, in most cases. Multiple studies show apixaban causes fewer major bleeds than warfarin in patients with moderate to severe kidney disease, including those on dialysis. One study of 127 dialysis patients found apixaban’s major bleeding rate was 1.8% versus 3.7% with warfarin. Warfarin also increases the risk of vascular calcification and intracranial hemorrhage in this group.
What if my creatinine changes after I start a DOAC?
Recheck your creatinine clearance every 3 to 6 months. If it drops below the threshold for your current dose, you may need to reduce it. For example, if you’re on 5 mg apixaban and your CrCl falls below 30 mL/min, switch to 2.5 mg. Never assume your dose is safe forever-kidney function can change quickly, especially in older adults or those with diabetes.
Can I take a DOAC if I have stage 4 kidney disease?
Yes, but the dose must be adjusted. Stage 4 CKD means CrCl is usually between 15 and 29 mL/min. Apixaban should be reduced to 2.5 mg twice daily. Edoxaban can be reduced to 30 mg daily. Rivaroxaban and dabigatran are not recommended at this stage due to higher bleeding risk. Always calculate CrCl using Cockcroft-Gault before making any changes.
Final Thoughts
DOACs are powerful tools-but only if used correctly. In kidney disease, the margin for error is thin. A simple mistake in dosing can mean the difference between preventing a stroke and causing a bleed. The key is to know the numbers, know the drug, and never rely on assumptions. When in doubt, start low and monitor closely. Apixaban is the safest bet in advanced kidney disease. And when it comes to dosing, Cockcroft-Gault isn’t outdated-it’s essential.
9 Responses
This is gold. Seriously. I’ve seen so many patients get screwed over because someone used eGFR instead of Cockcroft-Gault. One guy got 5mg apixaban twice daily even though he was 82, 58kg, and had a creatinine of 1.7… ended up in the ER with a retroperitoneal bleed. ABCs saved his life when we caught it. Always check the numbers. Don’t trust the auto-fill.
Ugh. Another ‘clinical guideline’ post that ignores real-world chaos. You think doctors actually calculate Cockcroft-Gault by hand? In a 12-patient rush? Nah. They glance at eGFR and click ‘standard dose’. And then blame the patient when they bleed. This isn’t medicine-it’s a lottery with anticoagulants.
It’s fascinating how we’ve institutionalized a 1976 formula as the gold standard while ignoring its limitations. The Cockcroft-Gault equation assumes a standardized muscle mass, yet we treat elderly patients who are cachectic, frail, or have low muscle mass due to chronic illness. Is it the formula that’s outdated-or our failure to contextualize it? Perhaps we need a recalibrated model that integrates biomarkers like cystatin C or bioimpedance. But until then, we’re applying a blunt tool to a scalpel problem.
Oh wow. Apixaban is ‘safer’ in dialysis? Really? Because the FDA hasn’t approved it? And you’re telling me we’re just winging it with off-label dosing? That’s not innovation-that’s medical malpractice waiting to happen. Next thing you know, we’ll be giving chemo by ‘gut feeling’ too. 😭
I work in nephrology. I’ve seen 3 patients die from DOAC overdoses because someone didn’t adjust. One was on rivaroxaban 20mg with CrCl 12. His family sued. The hospital settled. Now I scream at every resident who says ‘eGFR is fine’. I’m tired. I’m angry. I’m done. 😔
The most alarming part of this entire issue isn’t the dosing-it’s the systemic failure to prioritize pharmacokinetic literacy in clinical training. We teach residents to memorize drug names and brand names, but not how to interpret renal clearance curves or understand the difference between glomerular filtration and tubular secretion. Without this foundation, no algorithm, no checklist, no ‘ABCs’ will prevent harm. We’re treating symptoms, not systems.
The data presented here is both compelling and sobering. It underscores the necessity of interdisciplinary collaboration in anticoagulation management. Virtual anticoagulation clinics, as referenced, represent a model of care that is not merely efficient, but ethically imperative. Their success rate suggests that the future of precision therapeutics lies not in individual clinician expertise alone, but in structured, team-based oversight.
Let’s be real: the pharmaceutical industry pushed DOACs because they’re profitable. Now they’re pushing apixaban as the ‘safe’ option for dialysis patients because they have the data to back it. But who funded those studies? Who wrote the guidelines? I bet it’s the same people who made billions off this. And now we’re supposed to trust ‘early data’? Wake up. This isn’t science. It’s marketing with a stethoscope.
In India, we rarely have access to lab-based CrCl calculations. Many rural clinics rely on estimated creatinine based on age and gender alone. We use apixaban 2.5 mg twice daily as default in elderly CKD patients-not because we know their CrCl, but because it’s the least risky option available. We adapt because we must. This isn’t ideal, but it’s survival medicine. We need global guidelines that account for resource-limited settings, not just US hospital protocols.